

Is it really true that folic acid is “bad” for you because it’s synthetic and your body must convert it to the metabolically active form of folate, L-methylfolate, before your body can use it? Or was this myth started to sell more expensive methylfolate supplements and inaccurate testing methods such as the MTHFR genetic test?
Proponents of methylfolate supplements often think that more is better, both in dose and duration. For many years now we have seen negative side effects from the use of all forms of folate and folic acid supplementation, and new research finally confirms what we’ve been sharing for decades: any form of folate or folic acid should not be taken long term without specific biochemical laboratory testing and evaluation due to the very negative side effects that could arise.
It is not only important to know who would benefit from taking folate, folic or folinic acid, or methylfolate and how much is beneficial, but also a need to understand which form is best for each individual.
What Is the Difference Between Folate, Folic Acid, and Methylfolate?
Also called Vitamin B-9, folate is naturally found in many foods including green leafy vegetables such as spinach and swiss chard, to beets and avocados. It helps us utilize proteins in our bodies, form new blood cells, and create new DNA. It is important for the prevention of neural tube defects in infants as well as heart disease. It is also needed to lower homocysteine, an amino acid that can be problematic when elevated.
In 1998, folic acid fortification of flour and cereal began in an effort to minimize neural tube birth defects. Doctors also began prescribing folic acid supplements, which are a way to take concentrated amounts of folate, to their pregnant patients. Unfortunatley, overprescribing became the norm (and continues to this day), which has lead to an increase in autism and mental health disorders in children such as ADHD, OCD, and cases requiring a depression and anxiety nutritionist to name a few.
The Duality of All Forms of Folate and Folic Acid Activity
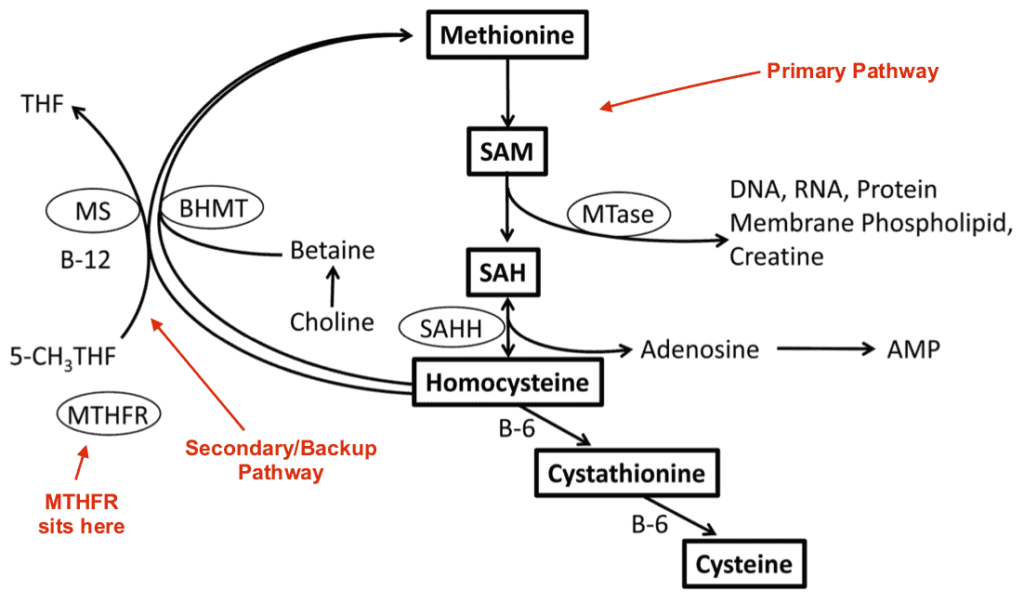
Much discussion surrounding methylfolate comes from genetic testing and the MTHFR paradigm, which is neither an accurate assessment nor an appropriate guide for true methylation disorders because the MTHFR test is only 30% expressive at best, which means 70% not expressive. Another misconception people have is that MTHFR is part of the primary pathway of methylation. MTHFR is a powerful methylating enzyme in a certain part of your system, but it’s part of a backup pathway, not the primary pathway.
Methyl groups control DNA by binding to a gene and telling it whether or not to express itself. I don’t know about you, but I’m not at all comfortable banking my health on something that might only be 30% expressive.
So what happens when you feed the backup pathway and not the primary pathway? Your backup is depleted and you plunge, and this is what we see happening all the time in people that take high doses of methylfolate. In fact, if you look at the Methylation Profile test by Doctor’s Data (which is what I use in my clinic) it specifically illustrates that MTHFR is part of the secondary or backup pathway, and it certainly does not play a prominent role in mental health.
Methylation status is determined by a tug of war, as we’ve said for a long time now, a tug of war between enzymes for undermethylation versus enzymes for overmethylation. The eight to 10 enzymes over here versus the 12 enzymes over here as groups, and whoever wins that tug of war determines your methylation status, not one enzyme. You may have a SNP (single-nucleotide polymorphism) but it doesn’t mean that that SNP is causing you any trouble. As a prenatal nutritionist, I prioritize looking at your functional biochemical status over a static genetic test; understanding whether that SNP is actually expressing is the only way to ensure your folate intake is supporting, rather than hindering, your baby’s development.
To learn more about MTHFR and methylfolate, check out my podcast episode below with Dr. Albert Mensah, Co-founder of Mensah Medical. You can also find the Eat For Life podcast on Apple Podcasts, Spotify, Google Podcasts, or wherever you listen to podcasts!
So Why Does Methylfolate Cause So Many Problems?
What many people fail to understand is the duality of all forms of folate and folic acid activity. One may take longer or faster to work, but they all end up doing the same thing over time, which can have a devastating effect on mental and physical health.
This is because in the cytoplasm (outside the nucleus of the cell), it’s a donor of methyl, so for an undermethylated individual (that doesn’t make enough methyl groups), the thinking is that MTHFR methylfolate is the appropriate course of treatment. In actuality, that’s not correct because in the nucleus, which is the command center of the cell, where we are trying to affect change, it steals 10 times more methyl than it donates. This can alter many cellular mechanisms including detoxification, enzymes, hormones, and neurotransmitters. This is because all forms of folic acid (including folinic, MTHFR methylfolate, and plant-based whole food sources such as spinach and avocados) steal methyl at the level of DNA.
This is why I don’t recommend vegan diets for undermethylated individuals.
Again, whatever form of folate or folic acid you take is going to work differently outside the nucleus of the cell where it actually donates some methyl into the system and this is one of the reasons MTHFR methylfolate has become so popular.
Yes, MTHFR Methylfolate Works Faster
The ready-made solution that so many clinicians use is “let’s just supplement with 5-methylfolate.” It certainly would be an open and shut case if biochemistry was as simple as this. But of course, things get more complicated, and this approach doesn’t usually work.
Loading up on 5-methylfolate, especially if given by itself will result in neurotransmitter changes, erring on the side of elevated glutamate, and shunted serotonin synthesis. It’s the reason so many people taking massive doses of methylfolate have such a high frequency towards adverse reactions and why so many people come to me with serious side effects from methylfolate supplementation.
Again, you need to address the entire pathway, not just one enzyme. So then the challenge with methylfolate, if given to an undermethylated person, is that the methyl piece acts and goes away and now you’re left with a demethylating agent. And as I shared previously, all forms of folate and folic acid donate some methyl outside the nucleus of the cell, but inside the nucleus, which is where our DNA lies and all our instructions are made, it steals 10 times what it donates in the cytoplasm.
Methylfolate is a nonfunctional creature. If you think about the methylation cycle, spinning millions of times in one second, do you know how often methylated folate actually works? One time. One time out of a million spins and it’s done for the day and this is why Dr. Walsh of the Walsh Research Institute calls it a suicidal nutrient. Methylfolate does not have the power most people think it does.
Folic Acid Supplements: Why Process Doesn’t Matter As Much
Most folks misunderstand the process involved in the metabolism of folic acid versus methylfolate. This is the key to understanding the difference between how folate gets into the cell, or the time it takes to do that, versus the end goal of having a physiological effect from taking the particular form of folate you have ingested.
Folic acid doesn’t have to be demethylated, but methylated folate does. Even though methylfolate gets into the system faster, it doesn’t actually begin to work faster than folic acid would because there is the extra step of demethylation before it can be utilized. It is only absorbed faster and still needs processing. Quicker absorption has to go through longer processing and can ultimately take longer to complete the utilization process.
It’s like the difference between taking a direct flight to a city and taking a connecting flight to the same city. There are more steps, more delays when you take a connecting flight that re-routes you through another city. One way takes longer. One way is more direct. Once something enters a cell there is a whole lot that goes on. Whether you take a direct route or a re-routed path makes little difference in the end. By the time it is all said and done these pieces are all moving in the same direction. The only difference we are talking about is the rate at which they are moving.
The Dangers of Methylfolate
Methylated folate is not a one size fits all folate supplement. For some, it can have adverse effects, and unless you are properly tested for your methylation status, you do not know whether it will be beneficial or detrimental to you.
What do you think happens to that methyl contained in methylated folate? That methyl is going to get absorbed into your body. I’ve already detailed what happens to an undermethylated individual taking methylfolate, but what if you give that methylfolate to a person who is overmethlyated? Well, it is like adding kerosene to put out a fire. You’ll make your methylation imbalance worse. Overmethylated patients should use folic acid that is not methylated. If you are overmethylated do not take methylated folate or any other product that is methylated.
But Folic Acid is Synthetic, and That’s Bad, Right?
Folic acid is synthetic, yes but this does not make it unhealthy. It works, and it works better than natural forms in most cases. Folic acid is used to fortify foods and is found in most dietary supplements, simply because it is more stable and bioavailable than natural folates. Historically, since the days of Carl Pfeiffer, the pioneer in orthomolecular medicine, we have traditionally used folic acid for our patients and it has shown to be extremely efficient and effective. The notion that folic acid is synthetic and is not effective is inaccurate.
Anytime you take something out of nature and take it into a lab it’s technically not natural anymore and has gone through processing and synthesizing to get it into pill form. This is the case for methylfolate, folate, folic and folinic acid.
Folinic acid is metabolically active, which means that folinic acid does not require enzymatic conversion before it can be utilized. Folinic acid can be found naturally in foods, but in order to benefit from folinic acid, it has to be prescribed in therapeutic doses for our patients. There are times when we may prefer the use of folinic acid to folic acid when we work with certain patient populations. Folinic acid has its best utility in autism nutrition support, as we have seen over the years of research and clinical practice at Pfeiffer Treatment Center, now closed, the Walsh Research Institute, the Mensah Medical clinic, and here at the Eat for Life clinic.
To learn more about the dangers of folic acid use and vegan diets for breast cancer patients, check out my podcast episode 14 below with Dr. Albert Mensah, Co-founder of Mensah Medical. You can also find the Eat For Life podcast on Apple Podcasts, Spotify, Google Podcasts, or wherever you listen to podcasts!
We have seen clinically time and again that people who are truly undermethylated do not do well on methylfolate after two to three months. In fact, to the contrary, many people report worsening of symptoms. In summary, we have three decades of research and patient outcomes (a biochemical database of over 3 million chemical assays) that support all we’ve been discussing regarding the benefits of the different forms of folate and folic acid, and their appropriate usage as well as challenges.
Please remember everyone is unique so let’s not generalize regarding folate and folic acid supplement use. There is only one you. Even if you are a twin, there is still only one epigenetic you.
Nutrition Counseling To Help You Thrive
In order to heal methylation disorders, I aim to identify and address the root biochemical causes and imbalances of your symptoms.
I offer a free 1:1 consultation to help you disconnect from the hype and the marketing jargon, and address the true source(s) of your discomfort. It’s time for your healing journey to truly begin.
References
Too Much Folate in Pregnant Women Increases Risk for Autism (Johns Hopkins Study)
Science Daily: Researchers found too much folic acid was just as detrimental as too little.
23 & Me article about MTHFR (with research links)
MTHFR ACMG Practice Guideline: lack of evidence for MTHFR polymorphism testing




48 Responses
What is the difference between methylated folate and folinic acid?
Folinic acid is metabolically active, which means that it does not require enzymatic conversion before it can be utilized. Methylfolate requires the extra step of de-methylation before it can be utilized.
Folic acid is subject to folate trap is it not?
No, please read the article again. This is explained within the various forms of processing.
Yes I always felt I did better on folic acid than methylfolate..
Im confused so confused. I hade a test done that said i had the mthr gene mutation. So what do I take ????
Hi Crystal – MTHFR testing isn’t an accurate method for testing methylation status. Here’s a short video that explains it
I will contact you after my consult with Dr Mensah
Whoever is reading this maybe should read what Dr. Ben Lynch has to say on the topic.
https://video.search.yahoo.com/yhs/search;_ylt=AwrTccyUn9I2OTFfMQRzZWMDc2M-?p=
Ben Lynch and folic acid on you tube or SHEI.com (folic acid is synthetic)
Over 40 years of human research and clinical patient outcomes by Dr. Albert Mensah, MD, and William Walsh PhD, about the benefits of different forms of folic acid and their appropriate usage override what you’ve shared. I encourage you to read this post in its entirety, especially the section where synthetic folic acid is specifically addressed. Folic acid is extremely efficient and effective. The notion that folic acid is synthetic and is not effective is incorrect. Anytime you take something out of nature and take it into a lab, it is synthetic. Methylfolate is not a better form. In fact, as this post explains, it is not a good option for both over and undermethylated individuals.
Hello Samantha,
I am currently being treated by a practicioner who has been trained by Walsh so I will also bring up this question to her.
I was tested being overmethylated and having (mild) pyroluria. I am on a regimen that includes methylfolate atm and I am not doing any better so far. I am feeling very tense a lot of times and certain supplements seem to make things worse.
Now that I read your post, I am thinking of changing methylfolate for folic acid, but I am wondering if the dosage has to remain the same.
Thanks for your answer.
Best regards,
Hans
I’m overmethylated and use folinic acid. (I am also treated by Dr. Mensah.)
I have an MFTHR snp and read about staying away from folic acid.
As shared in this article that Dr. Mensah and I wrote together, folic acid isn’t bad and works quite well for patients that need it. Folinic is more metabolically active so we use it as well, again depending on the patient’s need and chemistry.
Hi, I might want to recommend your recipes for our customers, but are your recipes for people with the biotype “undermethylation” all low-folate?
One comment: According to Walsh, folate act as a serotonin reuptake promoter, driving serotonin activity even lower, and the benefits from improving methylation (if any) are overwhelmed by weakened serotonin neurotransmission for these persons. We have noticed mild depression from taking only 100-200 mcg of methylfolate for extended periods, so taking several hundreds or even thousands of mcg on a daily basis does not sound good. Still it is prescribed for many depressives with MTHFR. However I see some advantage of helping in the conversion of homocysteine to methionine, and other functions, but more is not better.
https://www.vitacure.me/blogs/news/methylfolate-the-suicidal-nutrient-dont-believe-the-hype
I am 8 weeks pregnant and an undermethylator. I had been avoiding folate for myself, but understand from Dr. Walsh’s writings that for the first trimester I should be taking methylfolate for the benefit of my developing baby, while continuing Sam-e and L-methionine for myself. I have been taking 400mcg of methylfolate and getting additional through foods. Do I need to revisit this? I have not been able to find a Walsh or Mensah trained practitioner in my area.
So what about a doctor who prescribes high doses of folic acid to women, like myself, when they are pregnant very early on in the pregnancy to prevent birth defects, and then we have a child with severe ADHD, on the autism spectrum, etc. Could this have contributed to that? I have no clue what my methylation status was at the time or is now.
Autism is a genetic and epigenetic condition. It is important to take folic acid in the beginning to protect your child, but not throughout pregnancy if you are undermethylated, as it can have negative effects. I encourage you both to get properly tested. Autism and ADHD are treatable, especially when caught early on.
I am reading up on the these old posts. Can you please describe what specific tests you think the parents should have done?
I am an under methylator (apparently down 40%.) I took folic acid prior to pregnancy and miscarried 3 times. This is one of the problems of taking folic acid for under methylation. Early 2017 I took a Genova test (Optimal Nutrition Evalutaion) which recommended I need 1200mcg of methylfolate. I have been doing this for 8 months now and feel great! Have also increased green leafy veg intake.
Hi Samantha
I’ve read your articles with great interest since reading Nutrient Power. I am going to be tested by a Walsh practitioner in Ireland (certified from WRI site so legitimate as I know many claim to be but are not) so I’m not looking for individual advice as I will get that in a few weeks once my tests are conducted and results come in. I just wondered generally about your opinion on the following
Ive heard Walsh say bloods are only part of the picture and in the books many traits are listed for each biotype -specifically referring to depression chapter. I feel I have traits from both under and overmethylated lists so to me tests are the only way to truly tell.
What I wondered is I had some tests on our national health service in the UK and have low folate at under 2.2 acceptable range seemed to be from 2.4- so lets say in theory I receive my Walsh tests back and and Im found to be an undermethylated person. Does this mean I should NOT attempt to increase my folates to an acceptable level as I know from reading the book undermethylaters should avoid folates.
Secondly and this is just out of interest how often do you have clients who seem to have traits from many of the biotypes? As I get the impression this is part of the decision making process Ive even heard Mensah and Bowman say in webinars they suspect what tests results will be before they come back and are normally correct. Whereas to me the bloods will reveal the true picture and when they come back the traits become irrelevant scientifically speaking as they are just generalisations vs chemical proof.
Thanks 🙂
If one wants to maintain b12 level but is a slow COMT+/+ methylator is it bad not to have some folate?
I’ve seen 50mcg 5MTF as a safe policy for b12 support in doubtful cases.
I’m compound heterozygous MTHFR, and I’ve never noticed problems with folic acid. I’m currently taking a B complex with both folic acid and cyanocobalamin, and it seems to be very helpful. I certainly am not inclined to seek out methylated versions that would be more expensive and not available locally…unless something changes.
Also, Ben Lynch lost all credibility with me when he basically equated folic acid with carbon monoxide in one of his videos. Comparing something that may not work for certain people to something that’s deadly for everyone was simply outrageous to me.
I am a little confused. Is this article still stating that all forms of folate are bad in undermethylated individuals and if not when and what type is helpful?
What about the research regarding excess folic acid in the bloodstream when the body is unable to convert it all, resulting in less folate getting into cells? Considering the average diet of fortified foods along with supplementation.
Have there been more recent findings that discredit this?
I take the Best Nest multivitamin which contains methylfolate and methylcobalamin. I am homozygous MTHFR for the C677T gene. This multivitamin helps me. Having the proper dose and formulation is key. This vitamin was created by a board certified neurologist.
Every specialist I have talked to says no folic acid if u have the Mthfr mutation.. but then again some drs believe the mutation is a major concern and others think it’s nothing.. I’ve had 6 miscarriages and because a Dr took my Mthfr mutation seriously I am now with a healthy child and staying away from as much folic acid as possible.. after dealing with everything I’ve been through I think folic for pregnant women with the Mthfr mutation is Kryptonite.. and so do many other specialists.
I have rheumatoid arthritis, and currently take a weekly dose of methotrexate. To offset side effects of this medication, I also take 1 mg daily of folic acid. I’m wondering if it would be advantageous to instead take folinic acid daily?
Folic Acid is NOT good for you if your body does not process it…please, get a blood test before you continue taking Folic Acid.
This topic is so confusing because you will read in one article that folic acid is SO dangerous and people should ONLY use methylfolate because they could have the gene mutation that doesn’t allow them to metabolize folic acid. Now this articles says the opposite.
I agree – so confusing. But no surprise since you can’t even find two doctors that both agree on whether an egg is good nutrition or it will kill you. I’m very fed up with the medical community that are supposed to base their care on science.
I have a question I was hoping you
(or others who read this) could help me with.
I have the 677T MTHFR mutation. I also have a history of 20 years with health problems and counting (toxicity / heavy metal toxicity / high ammonia problems).
Because of this I have tried on multiple occations to start up Metafolin as many suggest.
My problem is that if I take a 400mcg tablet, crush it, and take less than 1/10th of the table (what amounts to 20-40mcg) I get such a bad migraine that I have to lie in for 2 days and call in sick for work.
People may think I am exaggerating, but I am not unfortunately.
So I have taken potassium, B12 in various forms, and B-complexes in tandem with my attempts and made sure my B12 levels are good before starting the Metafolin – but this does not make a difference.
So my questions are:
1. Any suggestions to what could be going on here?
2. Is it a realistic alternative that I simply cannot tolerate methylfolate
(I am pretty confident it is not an allergic reaction) ?
3. In my particular situation: could folinic acid be a better alternative, and if so, what dosage should I start at
(since I have read that some of folinic acid gets converted to methylfolate in the body) ?
3. I consider buying the Metabolics B-complex drops, and titrating extremely slowly up from miniscule dosages like 5-10mcg of Methylfolate. Is this a good idea or a bad idea given what I described above? Your article seems to suggest it could be a bad idea right?
Kind regards
In Spain, the prevalence of the MTHFR 677TT genotype has reportedly approximately doubled in the population since the introduction in 1982 of folic acid supplements for women in early pregnancy
In USA
Folic acid fortification started heavily in 1992.
Autism began to quickly rise in 1993.
In the early 1990s, autism diagnoses began to soar. In the 10 years between 1993 and 2003, the number of American schoolchildren with autism diagnoses increased by over 800%.
DON’T USE FOLIC ACID, it’s absolutely toxic to your folate receptors in brain
Thank you for sharing with our community.
My daughter just had her blood work done revealing her Whole Blood Histamine level was 81. Indicating she is an undermethylator. She is looking for information to help her better understand methylation. In addition, provide information where she can read any published peer reviewed articles on the subject, more specifically undermethylation. Clinical trials would be helpful as well.
She is also wanting to start a family soon. There is some confusion about whether or not she should be taking any version of folate. Folinic Acid is mentioned as a possibility. Yet, Dr Walsh mentioned in his video that all folates aren’t good for undermethylators, or maybe just a small percentage of them???
It’s all very confusing as to know which direction of mindset to take with this!!!
Any information is truly appreciated!
Thank you,
LH
Thank you for publishing this and for your podcast. It helped me narrow down methylfolate as a major contributor to my son’s severe ADHD symptoms. He is seven, and he has been on multivitamins with high doses of methylfolate since he was 18 months old. It was interesting that your podcast implicated folate supplementation as a possible cause of the “terrible twos” because we thought we were experiencing those terrible twos with our son. His PCP & orthopedist recommended the multi after he fell and fractured both bones in his wrist, and they never questioned the high dose of methylfolate in the vitamins.
Our son was a premie and was born with a severe case of hydrops fetal is due to a lymphatic leak. He was not expected to survive, and he beat all the odds. He has been mostly healthy since that time, but the ADHD symptoms, along with aggressive and oppositional tendencies have progressively gotten worse with time. We are a firm believer in wholistic treatment, and have been afraid to seek the help of anyone in traditional medicine because we were concerned that he would be put on medication. We were saving that as a last resort because my gut intuition was that there was something causing this that could be rooted out. I’ve shied away from most Integrative doctors because their boutique-style practices are extremely expensive. Most sell off the shelf supplements, which I feel is both a conflict of interest and aren’t targeted enough to treat and address specific problems.
In our search to help our son, we began reading a book by Dr Greenblatt called Finding Focus. It offers an integrated approach with nutrient supplementation to help alleviate ADHD symptoms. We started following his recommendations, and we had great success almost immediately. We couldn’t believe that it was working so quickly. But, the piece of the puzzle that wasn’t addressed in the book was actually the missing piece. With all of the extra zinc, magnesium, B6 and omega 3 supplements we were giving, we were looking for a way to reduce the number of pills & capsules that our son needed to swallow. So, we took him off of Mercola’s children’s chewable multi’s and started a liquid multi that was entirely food based. Our son’s ADHD symptoms improved dramatically. He was a completely new child. I couldn’t believe it.
His last remaining problem was bedwetting, and I read an article about B12, folate and bedwetting on Ben Lynch’s blog. Because the liquid multi didn’t provide vitamin dosages, we decided to try the Seeking Health Children’s Optimal Multivitamins. Within days, our son’s ADHD, aggression and oppositional symptoms returned, and they seemed worse than before. So, we started comparing the ingredients and dosages in all of the vitamins. Mercola and Seeking Health both have extremely high doses of methylfolate, so I began researching side effects of methylfolate. I was astonished to find that the side effects mimic ADHD symptoms. Then, I began looking for everything I could find on the topic. Your blog, as well as a few other blogs came up that describe Dr Walsh’s findings on undermethylaltion. I was suddenly astonished that there were no warnings on these vitamins that are produced by seemingly reputable sources. How on earth was I supposed to know that a multivitamin was harmful to my child? I am angry and devastated that my son has had to endure the feeling of being out of control for his entire childhood, up to this point. And, I am now on board with your notion that it is better not to supplement at all, rather than overloading on nutrients that can be harmful to both physical and mental health.
Thank you for making this information publicly available. Without it, and without people like you who are readily sharing it online, I’m not sure that I ever would have found the right direction in which to turn. We have made an appointment with a Walsh Institute trained physician in our area and will soon be seeking out your services to help get our family on track for optimal mental and physical health.
Thank you so much for sharing your story! It’s unfortunate all the misinformation available today. Methylfolate is definitely not for everyone.
So because folinic acid does not require de-methylation does it not cause cellular undermethylation?
Hi Sami,
Is there ever a time when Niacin would be good for an undermethylator?
If you find that you are eating something that contains methyl folate , would you necessarily have to eliminate that? Or is the poison in the dose? If you keep that methyl folate to under 500mcg will you be okay?
Hi Naomi – methylfolate only comes in supplemental form. Food-based sources contain folate and yes, staying under 500mcg per day is safe if you are undermethylated.
Should i supplement with folic acid if i am geting 5000mcg intramuscular b12? What would be the ideal ratio? Unfortunately my doctor didn’t order folate tests but I know that I react extremely badly to methylfolate so I would have to supplement with regular folic acid.
This such an interesting topic.
Sami, could yo provide details on how and what to test for under/over methylation whether in or outside the US please?
Thank you.
@Sami G. I do apologize for misunderstanding your article and for criticizing. There is much good info there and I am relieved to know you see the overall picture. Thanks for advising that the folate supplement (methyl folate) is not for all people all the time. From the advertising, you would think it is some kind of miracle which everyone should avail himself of.
Hi Samia,
I really appreciate your kind reply. You said it best and the reason behind my desire to set the record straight: “From the advertising, you would think it is some kind of miracle which everyone should avail himself of.” And an expensive “miracle” at that… 😉
If I’m under methylated and eliminate all folate supplements, what should I be taking to circumvent my issues? Methionine? Sam-e?
Hartstikke bedankt Samantha,
Eindelijk iemand die mijn vermoedens bevestigd. Folaat alsook b- complex en multivitaminen stonden mij instinctief al tegen.
Ik slik echter wel b2 daar ik vanwege geen zuivel kunnen verdragen deze op dagelijkse basis veel te weinig binnen krijg.
Hoe zit het met choline en biotine? Deze heb ik om andere redenen nodig zoals vetverwerking, haar, huid, nagel isseus . Maar toch ook een methyldonor? Is dit dan wel verstandig om te nemen?
Aangezien ik op gekookte eierdooiers (wellicht ook door de hoeveelheid b vit en ik at er een tijd 5 pd)begon te reageren en mij afvraag of ik dit voldoende binnen krijg.
Nogmaals hartstikke bedankt. Jammer dat ik u nu tref nu ik financieel niets meer te investeren heb. Wellicht in de toekomst mocht dat mogelijk zijn ivm dat ik uit NL kom..
Ben echter al een eind op weg. Veel zelf in verdiept en health care en voedingsleer achtergrond. Dit aangezien de meesten met adviezen komen waarvan mijn gevoel zegt dat het niet goed is en bij mij erin verdiepen dit over het algemeen ook juist blijkt.
Kind regards,
Patricia
Undermethylted? Overmethylated? Properly methylated?
What is going on here. Let us not blame everything on genes. How is it that some women, like me, never took any supplement whatsoever, neither methyl-folate nor folic acid, and neither did my mother or grandmother – and none of us birthed defective babies. And there were thousands of women in the same category – they didn’t take anything but food. And some consumed alcohol and tobacco, and they birthed OK kids, who never exhibited any neurological problems or strange, violent behaviors.
I think there must be something going on here that so many are apparently under- or over-methylated. My guess is some sort of overall toxicity, not those ever-handy” genes”. That toxicity could be caused by vaccines of every and all kinds, as well as a decline in overall health, the details of which are impossible to sort out, as there are just too many variables.
Yes, it was at a certain time in history when they began adding folic acid to food and doctors began prescribing folic acid. So, a direct line has been drawn between autism and folic acid supplementation. However, I could draw a direct line between vaccines and autism, too – and I would not be incorrect. Vaccinating babies and children was ramped up during the period in question as well. Vaccines = mercury or aluminum, straight into the blood and brain. Also, neither I nor my mother or grandmother were ever vaccinated for anything except me for polio when I was 6 years old, but my mother and grandmother had nothing.
Folic acid might not be the culprit after all. I am not saying it is safe or unsafe, merely that there might be something else going on, namely overall toxicity, from a toxic world, which will lead to various deficiencies. This is why prospective parents should do some detoxification for at least a year before conceiving, with the input of reliable medical practitioners. Of course they never do, but it’s a suggestion.
Let us look at overall health, shall we, please. What I observe is a tendency to see only the trees and not the forest. Thanks for reading.
Hi Samia,
The title of this post is “MTHFR Methylfolate vs. Folic Acid: Facts and Myths,” hence the emphasis on genetic and epigenetic factors related to folate. I’ve never claimed these are the only factors, but when writing about a specific topic, it’s best to focus on it to avoid overwhelming readers.
In fact, I’ve long maintained through my podcast and blogs that there are multiple underlying factors contributing to autism and mental health issues, including genetics, epigenetics, stress, trauma, abuse, poor diet, gut inflammation, enzyme dysfunction, environmental toxins, vaccines, and more. However, this post addresses a particular topic to better inform people about a commonly misunderstood nutrient (folate) and the highly flawed MTHFR test.
So, let us be mindful of the focus topic before jumping to conclusions about what the author (me) is conveying.